What is Composite Bonding?
Composite is a tooth-coloured resin-based material used to improve the appearance of your teeth by closing gaps, fixing chipped teeth and improving their colour and shape. It is available in a wide variety of shades and can be matched seamlessly to your natural tooth colour. It can replace tooth surfaces that have been worn down and are also used to fill cavities in both front and back teeth.
Composites have been used for decades in dentistry but the reason it has gained popularity in recent years is largely related to the rapid advancement in developing modern versions of composite materials and methods of bonding these materials more reliably to tooth surfaces. These newer composites polish to a much higher shine, which is far more comparable to the lustre and surface texture achieved with porcelain than ever before.
There are many different types of composite bonding available and these can be categorised based on which surfaces are covered, the technique used to place the bonding and the level of planning required prior to placing the bonding.
Edge Bonding
This can be used to create smoother more even edges of the teeth but does not cover the front surface of the tooth. Edge bonding blends seamlessly with the existing colour of your natural teeth. Tooth whitening can be carried out ahead of time if you wish to enhance the colour of your teeth prior to having edge bonding carried out. Edge bonding will not mask the positioning of your teeth or make them appear straighter; it will only impact the look of the biting edges of the teeth. If your teeth are straight but the edges are slightly uneven, with minimal tooth wear, edge bonding may be a suitable option for you.

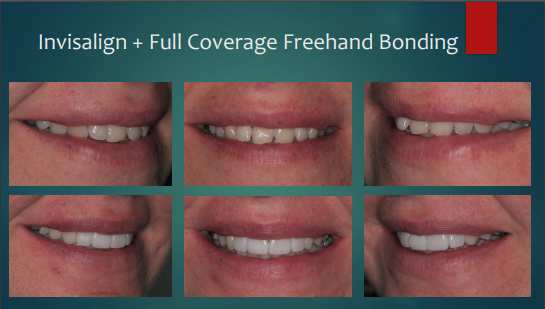
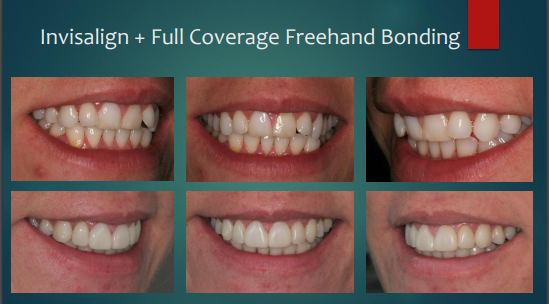
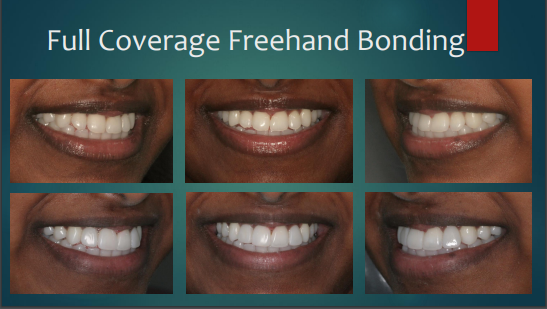
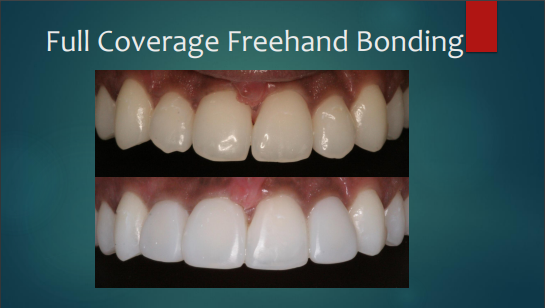
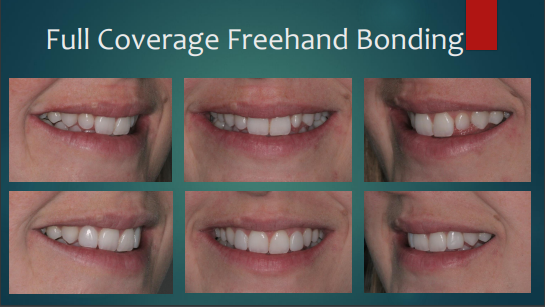
Full Coverage Freehand Bonding
This covers the full front surface of each tooth and their edges to ensure a truly even appearance, of both colour, opacity, and a reduction in the build-up of staining due to the absence of a visible join between the bonding and your natural tooth. It also allows us to build the front surfaces of the teeth out, creating a fuller smile and masking the areas that are not straight and filling the spaces between the teeth completely from the gum line down to the tooth edge and reshaping the spaces between the edges of the teeth. It can give the appearance of straighter teeth as well as close the gaps, however, the teeth would still need to be relatively straight.
Only minor rotations and spacing would be able to be masked with full coverage freehand bonding. If any changes in your bite are required, this type of bonding would not be suitable.

Guided Full Coverage Bonding
This type of bonding uses a different technique and allows your bite to be altered if required. This is most suitable in moderate to severe tooth wear cases and can rebuild all the surfaces of the tooth, not just the front.
Most commonly, this type of bonding will cover the full front surface of the tooth but can also wrap around the back surfaces if required. This would usually be indicated in circumstances where the tooth surface has worn significantly on the back surfaces of the teeth and can provide protection against further wear. The cause of the tooth wear must first be determined before undergoing any type of restorative treatment.
Due to the complex nature of reorganising your bite with these restorations, some occlusal (bite) planning and a trial smile stage would be necessary for this level of intervention. It allows us to “test” your bite before the final bonding is placed and ensure you will be able to tolerate it. It also provides you with the opportunity to see how your new smile will look prior to definitive placement and to ensure you are happy with the proposed final outcome regarding the aesthetics of the most important and most visible part of your smile. When the inside surfaces of your teeth are built up, you may notice some changes to your bite, which will be managed using the “Dahl Principle” (see below)






The Dahl Principle
In some cases, when your anterior teeth are restored to their full height you will notice that your back teeth do not touch to begin with and most of your chewing will need to be done with your front teeth. This usually takes 8-12 weeks to resolve, by which point your upper and lower back teeth start to meet again, making your bite feel more even, comfortable, and balanced. This is called the “Dahl Principle” and is a widely recognised method of reorganising the bite in the case of anterior tooth surface loss. Your bite will be checked at 3 monthly intervals following your treatment until it has closed completely. Some minor bite adjustments may be required along the way.
Whitening
Composite bonding is usually carried out in conjunction with tooth whitening so that the bonding can be matched to the new shade of the teeth. Naturally, teeth are often discoloured to different degrees, meaning all your teeth are not the same colour. Even if you are happy with the colour of your teeth, tooth whitening is still recommended to achieve a more uniform outcome. This way, the composite bonding will all be provided in a single shade, to match your natural teeth. Teeth planned for full coverage bonding are also recommended to be whitened ahead of treatment as composite is made to show some of the natural tooth colour though the material to make it appear as natural as possible, therefore darkly coloured teeth will show through composite layered over them and compromise the aesthetics of the final result.
A minimum of two weeks must be left between your last whitening application and your bonding appointment to ensure the best possible bond strength is achieved.
Benefits of Composite Bonding vs. no treatment
- Improves the aesthetics of your smile.
- Full coverage bonding can provide support to the underlying tooth tissue and protect the surfaces it covers from further wear, thinning and chipping.
- Can improve the occlusal (biting) relationship.
- Can reduce overclosure due to tooth wear.
Benefits of Composite Bonding vs. other treatments
- Less invasive than most other restorative options, e.g. porcelain restorations such as veneers or crowns.
- Less risk of nerve damage/devitalisation/need for root canal treatment when compared with crowns or veneers.
- More easily adjusted than porcelain restorations.
- Easily repaired.
- Will not cause wear of opposing tooth surfaces – a known risk of porcelain restorations.
- Avoids loss of further tooth surface as no significant preparation (filling/drilling) of the teeth is required.
- Quicker than orthodontic treatments, e.g. Invisalign/braces.
- Enhances tooth shape as well as addresses colour and staining issues, unlike ICON whitening and resin filler system.
Material Risks of Composite Bonding
- Less stain resistant than natural healthy tooth surface and porcelain.
- Requires regular polishing (annually) to maintain its initial lustre and shine. Polishing removes a small amount of thickness of the bonding each time, meaning eventually the whole restoration will require replacement.
- Shorter lifespan than porcelain (i.e. every 5-7 years rather than 10-15 years for porcelain).
- A minor amount of tooth tissue is removed when “texturizing” the tooth surface prior to bonding and when bevelling and smoothing edges to create seamless joins between tooth and composite, meaning this procedure is not completely reversible but still preserves as much tooth as possible.
- Poor oral hygiene around any type of restoration on a tooth (including composite bonding) can lead to complications of tooth decay and deterioration of gum health.
- Colour or staining of the natural teeth will not be sufficiently masked by composite material and may compromise final aesthetic outcome, particularly if the teeth are not whitened sufficiently prior to treatment.
- A tooth that has been traumatised by an accident or has had deep decay in the past may have experienced damage to the nerve of the tooth. This may not be obvious at the start of the treatment as quite often there are no obvious symptoms or signs. If the tooth were to become symptomatic after treatment, further treatment may then need to be carried out on this tooth. Root canal treatment may be required (at extra cost).
- Composite can chip and fracture, particularly when eating extremely hard or crunchy foods or if you grind your teeth. The use of a mouth guard at night significantly lowers the risk of fractures occurring.
Limitations of Composite Bonding
- Composite bonding is not appropriate for moderately to severely misaligned teeth. If teeth are not relatively straight prior to bonding being placed (with the exception of minor rotations, crowding or gaps), the aesthetic outcome will be severely compromised. It may create an obstacle for cleaning well between the teeth, which may eventually lead to tooth decay or deterioration of the gum health in the surrounding areas.
- If oral hygiene is not acceptable to receive any form of ‘cosmetic’ dental restoration (too much plaque/not brushing/flossing enough/inflamed gums) then composite bonding will not be an appropriate treatment modality. Stabilisation of oral health would need to be achieved first.
- If there is no room for any incisal-edge lengthening in the current occlusal/incisal scheme (biting position) this is a complex case and would be more suitable for a full-mouth rehabilitation which would include restoration on the back teeth also.
- If your gum levels are uneven you may benefit from Laser Gum Contouring prior to your bonding appointment to ensure the most even and aesthetic outcome.
- Some areas of the tooth may require Enameloplasty (reduction of minute amounts of enamel, i.e. <1mm) to improve the aesthetic outcome/dimensions of your composite bonding.
AFTERCARE
You should be made aware that ongoing dental care is particularly important following any type of aesthetic treatment. Regular check-ups, hygiene visits and a good oral hygiene regime at home, in addition to wearing a retainer at night, will be essential to ensure your smile looks as good as possible for as long as possible. You will need to invest time in cleaning and flossing your whole mouth daily. An appropriate regime for this will be advised on the completion of your treatment. You may wish to top up your whitening (see above for details) to keep the colour of your teeth that do not have bonding covering them at its best.
Preventing Staining: Composite bonding is more readily stained by coloured foods and drinks (e.g. curry, tomato-based sauces, tea and coffee) than porcelain or natural tooth. In the first week after your bonding is placed you are advised to avoid any brightly or heavily coloured foods for at least 2 weeks. You will return for a final polish two weeks later, after which you may resume a normal diet.
Polishing: You are recommended to have polishing carried out annually with your dentist to keep your bonding looking its best for as long as possible.
Mouthguard: This will protect your composite bonding overnight when grinding and clenching forces can cause the composite to fracture. If you take up the option of having a mouthguard made to wear at night (provided at a fee of £250 for three) any repairs required within the first year will provide free of charge. Any repair work required beyond this time scale will incur a fee, which will depend upon the extent of work required. We recommend having three mouthguards made at the same time as they are better valued for money than having replacements made in the future, and so that you have spares available in the event of loss or damage to your existing mouth guards. Mouthguards can also prevent minor movements of the teeth in the coming years.
Future Replacement: Composite bonding is an irreversible procedure. Once the material is bonded to the tooth it can only be removed by carefully drilling it away from the tooth. Preventing minor damage to the underlying tooth during the removal process cannot be guaranteed. Composite restorations will require repair, maintenance and ultimately replacing at some point in the future as they will not last forever. Once the teeth have full coverage composite bonding they will need new replacements in the future at some point (usually every 5-7 years). You must be aware of the future cost implications for this.
PAYMENTS
We take 50% of the total payment due for each appointment as they are booked to secure the booking. If you wish to, you may apply for a 0% finance agreement to facilitate payment over a longer period than your treatment would take to complete.
WHAT HAPPENS NEXT?
Please take time to consider your options and feel free to call or email me if you have any queries. If you wish to proceed with treatment, please let us know which treatment option you wish to undertake, and we will arrange the necessary visits.
*All photographs obtained and displayed with appropriate consent from patients. All treatment shown in sample cased included in this document carried out by Dr Davina Philips at Pennypot Hythe.